
Xue Wen, Peng Lei, Shengxin Huang, Xiaoyu Chen, Yanchi Yuan, Di Ke, Rui Liu, Jiaxi Liang, Erqi Wang, Bo Wei, Kedi Xiong, Sihua Yang, "High-fluence relay-based disposable photoacoustic-ultrasonic endoscopy for in vivo anatomical imaging of gastrointestinal tract," Photonics Res. 11, 55 (2023)
- Photonics Research
- Vol. 11, Issue 1, 55 (2023)
Abstract
1. INTRODUCTION
Neovascularization and membrane proliferation are common signs of gastrointestinal (GI) tumor or inflammation formation [1]. Tissue biopsy is a standard procedure to reveal the histopathology of biopsy samples taken from the superficial epithelial layer. However, tumor invasion and fibrostenosis disease cannot be effectively evaluated by mucosal biopsies since they generally occur at deeper layers of the digestive wall [2–5]. The vascular morphology is clinically standardized for cancer staging and surgical strategy formulation by narrowband imaging combined magnification endoscopy [6,7]. Nevertheless, the optical imaging depth is limited to the superficial mucosa, and the vascular morphology in the deep mucosa has been a dead zone. Different from optical imaging methods, photoacoustic imaging (PAI) provides angiography-specific imaging with high penetration and optical resolution (OR) [8–17]. In the previous studies, PAI through the whole thickness of intestinal wall in animals and humans has been demonstrated [18]. PAI combined with ultrasound (US) imaging has embodied inherent advantages for clinical GI endoscopy, providing full depth of view of the membrane layer structure and microvascular angiography [19–23].
For the application of photoacoustic endomicroscopy (PAEM), two subcategories of a side-viewing PAEM catheter, distal-driven and proximal-driven, have been constantly innovated [24–30]. The proximal-driven catheter is increasingly prominent and accounts for its miniaturization and low manufacturing cost. The proximal-driven catheter is driven by a scanning device to make a probe rotation and retracement inside the imaging window (IW) tube for three-dimensional (3D) imaging. Whatever that model of catheter is, to avoid cross infection and increase working efficiency, disposable imaging catheters are the workhorses in current GI examination, which is flexible and convenient in clinical settings as disposable medical consumables [31].
A disposable imaging catheter must be catheter-switchable, self-internal 3D-scannable, and system-repeatable. In recent years, most of the PAEM catheter systems have been implemented based on mechanical scanning. Nevertheless, numerous PAEM catheters have been limited to acoustic resolution because the optical waveguides relied on large-core (
Sign up for Photonics Research TOC. Get the latest issue of Photonics Research delivered right to you!Sign up now
One of the great challenges that prevent the OR-PAEM catheter from being disposable is low optical coupling efficiency and the power damage threshold of optical coupling junctions based on SCF. In order to achieve the switchable PAEM catheter, the integrated optical and electrical interface is inevitable. From the laser to the imaging catheter, there are two essential optical cold junctions in the optical path, stator to rotor, rotor to independent catheter. However, the SCF-based PAEM catheter at the wavelength of 532 nm presents considerable difficulty for optical coupling [33,35]. First, SCF with a small mode field diameter is vulnerable to laser damage with high peak power. Therefore, the flanged fiber docking leads to a high local power density, posing a threat to the end face. Second, the coupling efficiency puts extreme requirements on the concentricity and gap distance of the pair of coupling fibers, bringing much insertion loss. The low damage threshold and coupling efficiency lead to insufficient energy to excite photoacoustic signals.
Another great challenge is the non-customized optical parameters of the imaging catheter. Working distance, depth of focus, and size of spot are vital parameters for evaluating the performance of the PAEM imaging catheter. However, with the conventional method, controlling the gap distance between the optics, it is hard to achieve an anticipant beam output with customable OR parameters. Thus, the previous approach of the distal optical strategy is empirical and unreliable for standardization.
In this study, a prototypic disposable PAEM-US imaging catheter and a power interface unit (PIU) were first developed for GI endoscopy. A 0.25 pitch GRIN fiber (GRIN-F) was isometrically fused to an SCF, named end-cap fiber (ECF), for collimated beam output. ECF-based optical rotary connectors (ORCs) and optical pluggable connectors (OPCs) were invented, realizing high-fluence optical coupling. Based on this, the PAEM catheter can be freely combined and separated from the PIU. At the distal end of the catheter, a 2.4 mm outer diameter (OD) mini-probe was designed to be collinear with focused light and sound for high sensitivity of PAI [37,38]. In addition, a focus-fixed PAEM catheter was designed with customizable OR parameters. In this article, our engineering strategies from the catheter to PAEM-PIU were described in detail, and the
2. METHODS
A. High-Fluence Relays for Endoscopic PAEM
There has been a long-standing expectation that the endoscopic OR-PAEM could be compatible with OR of SCF as well as the optical coupling fluence and end-face damage threshold of LCF. In this study, ECF was first applied for OR-PAEM to overcome the challenge. An ECF was fabricated based on a 0.25 pitch GRIN-F (100/125 μm, GI2013-N, Changfei, China) and a long SCF (9/125 μm, PM-TSF-9/125, Nufern, USA) [Fig. 1(a)]. Figures 1(b) and 1(c), respectively, display the microscopic end face of the SCF and GRIN-F. Different from total reflection in the SCF, the optical waveguide in the GRIN-F presents a sinusoidal distribution due to its GRIN of fiber core. Theoretically, a point source incident beam will exhibit collimated light at 0.25 pitch length, which is preferred for optical cold coupling and beam shaping. According to the principle of optical path reversibility, a pair of ECFs can work together to form a coupling relay [Fig. 1(e)] for optical cold coupling. The prime relay consisted of the ECF, C-lens (N-SF11, Gongxin Photoelectric Technology Co., Ltd., China), and total reflection prism (H-ZF62, Jingliang Photoelectric Co., Ltd., China) [Fig. 1(f)]. Focus-fixed beam was achieved for OR-PAEM, whose depth of focus and spot size are determined by the radius of curvature of the C-lens. ECF-based optical strategy was first applied in the PAEM system [Fig. 1(d)]. A 532 nm pulsed laser (Mosquitoo X 532-2-V, InnoLas) was applied as the PAI source, and the output laser at a repetition rate of 30 kHz was spatially filtered and coupled into SCF by a fiber port coupler (PAF2-7A, Thorlabs). Subsequently, the optical waveguide went through the first rotary coupling relay (a customized ORC, Thread Photoelectric Co., Ltd., China) and the second pluggable coupling relay (a lab-built OPC). Finally, the laser was delivered to the distal end and reshaped by the prime relay. For the ORC, the optical path must be divided into the rotator and stator due to the requirement of proximal-driven mechanical scanning. For the OPC, the optical path was divided to the PIU side and catheter side, which means that the PAEM catheter can be independent of the PIU. The flange is a common device for fiber optics cold splicing, while SCF-based optical coupling introduces significant insertion loss. Worse still, the instantaneous power density at the fiber end face is too high for the small mode field of SCF, which leads to the collapse of end face. The neat facture of ECF captured many advantages. First and foremost, the power resistance has been significantly improved. Since the mode field diameter is increased tenfold, the laser damage threshold was optimized hundredfold according to the estimation formula of end laser damage threshold [39]:
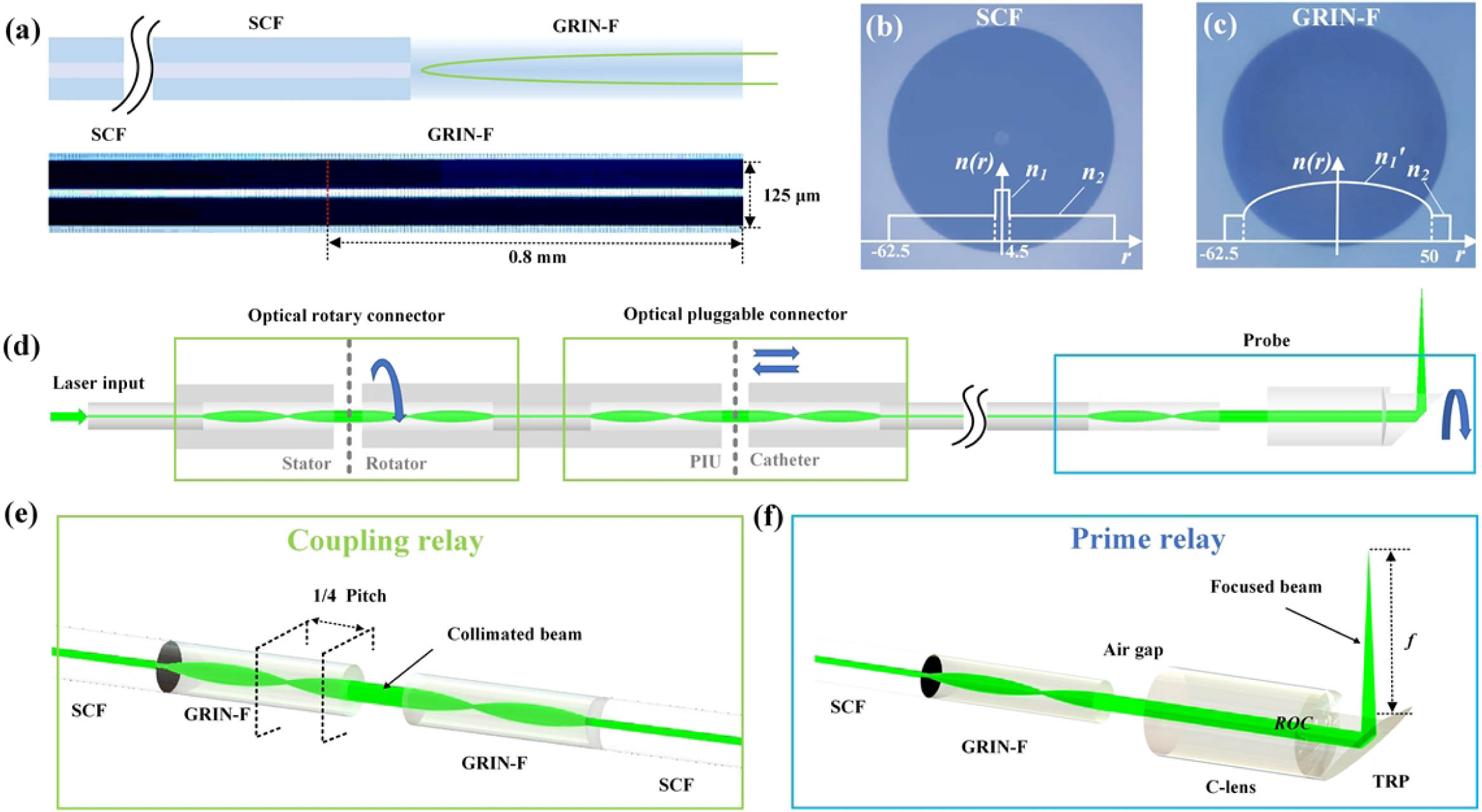
Figure 1.ECF-based optical waveguide strategy of endoscopic PAEM system. (a) Schematic diagram and photo of ECF; 0.25 pitch (
B. Collinear Designed PAEM-US Mini-Probe
An important aspect of PAEM for clinical applications is that the PAEM can be combined with US for co-registered images. As vividly depicted in Fig. 2(a), the PAEM-US mini-probe performs 3D helical scanning for PA and US imaging under the video endoscope. Stratified structural morphology can be inverted by US mode, and depth-resolved angiography can be exhibited by PA mode. The miniaturized structure of light transmittance and sound reflection is applied to realize the collinearity of sound and light for optimized sensitivity [Fig. 2(b)]. The focus-fixed beam passes through the sapphire glass and illuminates biological tissue. PA and US waves are reflected by the 45° tilted sapphire glass and harvested by a front-mounted transducer. A high-frequency transducer (38.5 MHz center frequency and 60.37% bandwidth, 1YT0032, Doppler Electronic Technologies Inc.) was used for simultaneous PA and US imaging [Fig. 2(g)]. The optical and acoustic components were assembled in stainless steel (2.4 mm OD, 13 mm rigid length). A Pebax tubing (2.55 mm ID, 2.7 mm OD, Bova Plastic Co., Ltd., China) was selected for IW, protecting the cavity from being injured by insulating the high-speed-rotating probe. Polytetrafluoroethylene (PTFE) tubes were selected for the interventional catheter with 2 m length. Driven by the PIU, 1:1 torque was transformed from the proximal to distal by a torque coil (2.3 mm OD, Asahi Intecc, Japan), and the mini-probe was rotated and retraced inside the IW tube for 3D imaging. The sharp edge of a surgical blade and tungsten wire (10 μm) was imaged with PA and US, respectively. By calculating the full width at half-maximum (FWHM) of the line spread function (LSF) and point spread function (PSF), the PA lateral resolution was evaluated to be 18 μm and the US axial resolution 63 μm [Figs. 2(e) and 2(f)].
![]()
Figure 2.Collinear designed PAEM-US mini-probe. (a) Schematic diagram of intra-instrument channel workable, PA, and US dual-mode imaging. (b) Schematic of PAEM-US probe with main integrated components. Inset, the section view. UT, ultrasonic transducer; TC, torque coil; S1, S2, sections 1 and 2; IW, imaging window; SG, sapphire glass; TRP, total reflection prism; SCF, single mode fiber. OC, optical channel; CC, cable channel. (c) Photograph of the fabricated PAEM-US endoscope; SUS, stainless steel. (d) Photograph of the mini-probe combined with upper electronic endoscope (2.8 mm ID channel). (e) PA lateral resolution. (f) US axial resolution. (g) Pulse response and frequency spectrum of the transducer. Fc, center frequency; BW, bandwidth.
Clinical disposable PAEM catheters must be systematically repeatable and engineerable with constant OR parameters. As illustrated in Fig. 3(a), a general method for obtaining the laser scanning beam is by controlling the intercept
![]()
Figure 3.Simulation and test of prime relay. (a) Schematic of SCF-based and ECF-based optical reshaping. (b) Simulated
The simulated results in Fig. 3(b) indicate that, compared to SCF-based optical shaping, a constant
C. PAEM-PIU and Disposable PAEM-US Catheter
PIU adapted with a disposable catheter is a standard configuration for clinical endoscopy. Figure 4 depicts the design of the PAEM-PIU and disposable PAEM-US catheter. The coupling relay was employed in the ORC and OPC for optical coupling [Fig. 4(a)]. The stator of the ORC was connected to laser. The rotator was fabricated as the F-interface, integrated with the electrical connector. The optical and electrical devices were integrated with a BNC-like housing, realizing simultaneous optical and electrical coupling by plug-in operation. The PTFE slider was driven by the retracting motor and screw rod, carrying the rotating parts to retract at 10 μm step intervals. The hollow shaft was driven by the rotating motor and synchronous wheel with a rotating speed of 30 r/s. For an optimized signal-to-noise ratio (SNR), a 50 dB low noise ring preamplifier was integrated with the rotator of electrical slip ring (H0835-06, Senring). The full view of the disposable PAEM catheter is shown in Fig. 4(b), and the side view of the PIU and catheter is shown in Fig. 4(c). The optical and electrical communication for PA and US imaging must relay on an integrated interface. Gold-plated pins were used for electronic transmission, and SC-type OPC was used for optical coupling. The optical and electrical connectors were concentrically rotated inside the retracement connector, retraced inside the shell connector together.
![]()
Figure 4.Prototypic disposable PAEM-US catheter and PAEM-PIU. (a) Diagram of PAEM-PIU. F-interface, female interface; M-interface, male interface; ESR, electrical slip ring; L, Luer connector. (b) Full view of the whole PAEM catheter. (c) Connection of the catheter and PIU. Inset, caps used to house the SC-type OPC and electrical pinholes. SC, shell connector; RC, retracement connector; EC, electrical connector; OC, optical connector.
One of the key achievements of this work is that ECF was introduced for PAEM for the first time to deliver a laser with high efficiency and stability. The low coupling efficiency and end-face damage threshold of SCF-based optical coupling bring a seemingly insurmountable challenge. Because of the high mechanical tolerance for concentric docking of 9 m core diameter, there is no high-fluence SCF-based ORC of 532 nm wavelength available. Attempts with an SCF-based ORC show an unstable and low coupling efficiency of maximum 60%. Another frustrating point is the low end-face damage threshold of SCF. After testing, the maximum permissible energy of the SCF-based cascaded optical waveguide for PAI is less than 450 nJ, which is inadequate to excite PA signal for high-SNR images. Furthermore, it is difficult to guarantee the service life due to the environmental factors (particulate matter, temperature, humidity, etc.). In contrast, the ECFs enjoyed a high coupling efficiency of over 90% and long-lasting power resistance of up to 10 μJ. Thus, the stepless variable energy can be realized for endoscopic PAEM. In this article, the
Energy Coupling Efficiency and Damage Threshold of OPC
| No. | SCF-Based | ECF-Based | ||||
|---|---|---|---|---|---|---|
| Coupling Rate (%) | Damaged (Y/N) | Threshold (μJ) | Coupling Rate (%) | Damaged (Y/N) | Threshold (μJ) | |
| 1 | 91.4 | Y | 3.0 | 94.5 | N | 10 |
| 2 | 91.1 | Y | 2.9 | 94.2 | N | 10.1 |
| 3 | 90.5 | Y | 2.9 | 94.6 | N | 10.1 |
Energy Coupling Efficiency and Damage Threshold of ORC
| No. | SCF-Based | ECF-Based | ||||
|---|---|---|---|---|---|---|
| Coupling Rate (%) | Damaged (Y/N) | Threshold (μJ) | Coupling Rate (%) | Damaged (Y/N) | Threshold (μJ) | |
| 1 | 63.4 | Y | 1 | 92 | N | 10.1 |
| 2 | 54.1 | Y | 1.1 | 91.8 | N | 10 |
| 3 | 57.5 | Y | 1 | 92.1 | N | 10 |
![]()
Figure 5.ECF-based coupling relay for ORC and OPC. (a) Schematic of the output laser beam of SCF and ECF. (b) 2D spot profile of SCF and ECF at the axial distance
3. IN VIVO ANATOMICAL IMAGING RESULTS
In order to demonstrate the system’s imaging capability, the colorectum of the Sprague Dawley rat (
The set of 2000 PA B-scans was stacked into the 3D volume rendering image [Fig. 6(a)]. Similar to most mechanical scanning imaging, non-uniform rotational disturbances (NURDs) introduced non-rigid motion artifacts in our results. We attribute this phenomenon to the non-uniform angular velocity due to the rotational friction. The Hessian matrix was used to restore the network morphology of the blood vessels and the maximum projection (MAP) of 3D data is shown in Fig. 6(b) with 1 mm relative depth encoded. It should be noted that the depth encoded results are not accurate in the fringe area of the transverse direction. Due to the curved surface coupling, defocus and non-concentric scanning occur in the scanning range where the tissue is separated from the IW tube, causing tensile distortion of the vessels and non-uniform depth projection at the border. Every 2 PA data points were intercepted for MAP, displayed in
![]()
Figure 6.
To further illustrate the depth morphological characteristics, every 10 PA data points (90 points in total) were intercepted for MAP, displayed in Fig. 7(c). The primary microvessels (dense mesh-like) are distributed in the superficial mucosa. Secondary (sparse mesh-like) and tertiary vessels (branch-like) are excavated as depth increases [34]. Data analysis and statistics were displayed in Figs. 7(d) and 7(e) by Angio Tool. Combined with the results in Fig. 6(g), the vessel diameter increases with depth, while the tortuosity of secondary vessels reaches its peak near the submucosa. The density of vessels decreases with increasing depth, evaluated by counting the number of vessel junctions and calculating the porosity. Data analysis and statistics of PA angiography are expected for future differential identification of tumor vessels.
![]()
Figure 7.PA depth-tomography results of rat colorectum. (a) Photograph of the rat colorectum imaging experiment. (b) Relative-depth encoded image with whole PA data. (c) Different depth of MAP view. (d) Statistics of vessel diameter and curvature as a function of depth. (e) Statistics of the number of vascular crossings and porosity as a function of depth.
In the
4. CONCLUSION AND DISCUSSION
Though adherent scanning of PA combined with US was successfully demonstrated by a prototype disposable PAEM catheter, there are still fundamental limitations in this study, including NURDs bringing slight motion artifacts, manifested as lightning-like lines in the axial direction. Post-processing of the image can repair the image to some extent, but it often takes a long time to execute, which cannot be corrected online to follow the pace of real-time imaging. We have found that the rigid length and quality of probe will affect the severity of NURD artifacts. In addition, the long rigid length of the PAEM-US mini-probe is not conducive to passing through the curved part of the natural lumen. The catheter design will be further optimized by using lens fiber instead of a lens assembly process. The rigid length of the probe can be further reduced to
The mini-probe was set in a water environment by water-injected structures. It is a distressing detail that, due to the non-infiltration effect, the tiny gap often traps air bubbles by normal fluid injection, affecting the propagation path of light and sound. In addition, in the
The angle view, depending on the effective contact area, was limited by the diameter of tube. In order to expand the angle view, shape-fixed panoramic endomicroscopy is promising for large digestive tracts by using a shaping balloon [40–42]. Under this scenario, the focus-fixed beam will be customized with focus positioned on the balloon wall, and the axis of the probe will be constrained to the center of the balloon for concentric scanning. The liquid-filled balloon will brace and reshape the intestines to a circle, and 360° angle view can be achieved.
The coupling relay maintains an excellent luminous fluence when the transmission wavelength is close to 532 nm. Benefiting from the high power-tolerance threshold, the scanning laser energy can be compensated by increasing the light source output. Thus, multispectral imaging of oxygen saturation and lymphatic vascular is feasible on the optical relays [43]. For the near-infrared wavelength (e.g., 808 nm or 1064 nm), dispersion-compensated fibers were considered to offset the positive dispersion.
In conclusion, a prototype disposable PAEM-US catheter and a PAEM-PIU were first developed for GI endoscopy. A fixed-focus beam with 3.4 mm working distance and 12.5 μm waist FWHM was customized for OR-PAI by freely combining ECF and C-lens. ECF-based coupling relay realized a high-fluence fiber optic waveguide. A coaxial structure was employed to ensure the collinearity of the optical and acoustic focus for an optimal sensitivity. The imaging capability of the system was demonstrated with
References


Set citation alerts for the article
Please enter your email address

© Copyright 2018-2021 | Chinese Laser Press. All Rights Reserved 沪ICP备15018463号-20